| Functions - Forms - Landscapes |




|
Notes on asylum architecture
Using the work of several people researching the history of function and form in the buildings and grounds used for psychiatric purposes. The index to the right will be developed as a means of finding ones way around.Extracts from Jacobi, C.W.M. 1841 On the construction and management of Hospitals for the Insane
" What is the most desirable situation for an hospital for the insane?We may presume, without further question, that the same circumstances, in regard to situation, which are found by a person who is free from any morbid tendency, to have a beneficial influence on his mental feelings, will generally, in some degree, contribute to the restoration of a mind diseased.
The establishment should be situated, then, under a mild sky, in an agreeable, fertile, and sufficiently dry part of the country, where the surrounding scenery, diversified with mountains, valleys, and plains, is calculated to enliven the spirits of the beholder, and invite him to wander and explore its beauties.
In the next place, there should be an unfailing spring of good drinking water, a running stream which will afford a constant supply for other purposes, and easy communication with some large market town, bestowing opportunities for procuring the necessaries of life, and for social and scientific intercourse.
So much of general attributes. As we descend into particulars, however, it admits of some doubt, whether, if the situation be left entirely to choice, it would be more advisable to erect the buildings of the establishment on a plain, or on an eminence; and whether they should be quite solitary, or contiguous to some town or village. And this certainly deserves some consideration.
A situation upon a moderate, easily accessible eminence, of from 150 to 250 feet at the highest, above the level of the nearest river, and commanding an extensive range of agreeable scenery, and an unconfined view of the heavens, is certainly productive in a mild and serene climate, of exhilarating and joyful emotions. Besides the advantage of a dry and salubrious atmosphere conferred by such a situation, it is not its least recommendation, that it enables the patients to extend their view far and wide, over the boundary walls or hedges of the estate, as these may be placed at the lowest purl, of the establishment. The patients are thus not so easily reminded every moment of their incarceration, and, through it, of their other miseries.
Whilst an establishment in a level situation is deprived of all these advantages, and must, therefore, generally cause a less kindly impression, both on diseased and healthy minds; still it enjoys other very important advantages, not possessed by the former.
The principal of these is the abundant supply of water, which a full stream affords for the baths, washing, and every kind of cleaning, as well as for the most appropriate construction of the privies.
Other advantages of a level situation, consist in the greater facility of enlarging the ground-floor of the buildings, to any required extent; in the greater protection from the influence of the winds and storms, thus materially affecting the consumption of fuel, and the ease of warming the day-rooms in winter; in the easier conveyance and delivery of all articles of consumption; and lastly in this, that the patients are more sheltered from the prying gaze of the inquisitive, to which they are too much exposed on a hill, which lies open to these glances from all sides.
All these advantages are met by exactly correspondent disadvantages which, in the situation of an establishment upon a hill can never be entirely overcome, and only even partially diminished, by a great outlay of money.
{fotnote: I cannot doubt that a piece of ground on a level with a running stream, would be, in general, a highly inexpedient site for a lunatic asylum in England. The dampness of such a situation in our humid climate - especially in the time of heavy rains, when the stream may lie swollen into a flood, is an irremediable evil which has no counterpart in an elevated situation, unless we speak of such an extreme height, as no one would contemplate for such a purpose. Besidcs there is scarcely any thing more important, in regard to the site of an asylum, than that it should afford a most complete drainage; and this can hardly be obtained, except in a somewhat elevated situation: and this character is by no mean' incompatilible with the advantage of retirement and shelter. (Editor)}
In the same way, the advantages and disadvantages at tending the entirely isolated situation of an establishment, and one contiguous to a town or large village, appear very nearly equivalent to each other. The neighbourhood of a market town certainly affords many conveniences and comforts, both in an economical point of view, from the promptitude with which various wants may be supplied, by the resident mechanics and tradespeople, and in other respects from the intercourse which may be kept up with the inhabitants. On the other hand, the vicinity of a town containing a population not entirely agricultural, but which consists-of mixed classes, is so annoying and inconvenient, from the intrusive curiosity excited by the patients, and the incessant scrutiny to which they are exposed at every step they take abroad; the difficulty of completely releasing them from the usual noise and tumult of society, however desirable it may be that many of them should enjoy this liberation, is so much increased, and so much facility afforded to the servants, and in some degree to the patients also, for carrying on forbidden intercourse with the inhabitants, that these reasons would compel me to select a situation nearly solitary. I should prefer, however, most of all, one in which the establishment should lie about half an hour's walk from a town. All the advantages to be thence derived, would then be within reach, divested of the prejudicial accompaniments of immediate contiguity.
Forms of asylumJacobi discusses the following "forms at present chiefly recommended for the buildings:Several distinct quadrangles having a certain connection and relation with each other. Examples: "the one at Ivry, the house for females at Charenton, and the large establishment at Rouen"..."All these were builit according to the maxims of the excellent Esquirol The one Jacobi describes was at Rouen: "The institution is adapted for three hundred patients, and intended to receive the incurable, as well as the curable. In front of the more ancient buildings, which had been used a long time previously as a lunatic asylum, five handsome quadrangles have been erected, one story high, containing the dwellings of the patients..." H form Example: Wakefield. The junction building has the "house- keeping" and common rooms for the use of both sexes and the two long wings are used one by the women and the other by the men. Lineal Form "in which all the buildings are ranged in a straight line... the domestic apartments are most properly placed in the centre... the divisions for the male and female patients...on their respective sides, in such a manner , that the convalescents and least deranged patients occupy the most distant wings." Examples: Bethlem (1815) and Perth Star or radiating Example: Glasgow Pavilions - [Pavilion is later used for a large, Florence Nightingale style building - We might call this early colony plan] "...it has been strongly recommended, that a certain number of distinct pavilions one story high, should be erected in a large piece of ground laid out like a park, and appropriated to the different classes of insane patients.... such an idea could only be realised in the case of a small private establishment, for twenty-five or thirty patients at the outside, and ... it would require a much milder climate than we are favoured with in Germany... An institution for two hundred patients, arranged on such a plan, would be so lost and dispersed on its own ground, that any regular superintendence and medical treatment of the patients would be impossible, even in the finest weather..." No Jacobi example. Compare Brislington House (1806) and the Colony Plan 1902 -1967 |
| Jacobi's model falls in the period where there are few examples in Susan Piddock's sample. Few of the asylums after 1845 met Jacobi's requirement of having 200 patients. One of these was Buckinghamshire Asylum . Cambridgeshire and Lincolnshire came close at 252 and 250 patients respectively. All favoured a linear layout, but none of the asylums followed Jacobi's suggestion of arranging houses around courtyards. Most met the requirements of a country location with the exception of Essex Asylum which was placed in the urban setting of Brentwood. While there was a strict separation of the sexes, the linear design meant that the various classes were visible to each other to some degree. Certainly all the asylums offered classification of the patients and small spur wards which could be used to separate the noisy and infirmary patients if necessary. As these asylums were for paupers there was no emphasis in providing different rooms for the various social classes as Jacobi recommended. |
|
Wakefield
Model of the original 1818 building made by Mr A.L. Ashworth, Hospital
Secretary 1961-1973, using the original plans and drawings fo the asylum
"The really old part of the hospital is shaped like an H where the cross piece has been extended on both sides so that it resembles two plus signs joined together. While the outside of the building preserves and eighteenth century dignity and balance, its plan is strictly functional, conforming to nineteenth century scientific theories of social control. This is in fact the 'double panopticon' which is to be found in so many prisons and places of correction - and mental hospitals - built at this period and for many years afterwards. Once having taken up position at one of the points of intersection, whoever is in charge can look anywhere, keeping an eye on things north, south east and west along the length of the four radiating corridors. Modern psychiatric nurses have never liked this arrangement. Apart from not being all that effective for 'ambulant' patients, it brings home the custodial role in a way that is nowadays felt to be unacceptable. This, however, is the architecture that they have inherited and must make the best of. |
|
Early - later adapted to corridor - Most early county asylums do not seem to have followed a typical plan. In most cases, however, a Corridor type layout was later adapted around them. I am assuming a date of 1810-1830 for these. Examples could be Nottinghamshire County Asylum (1810), Norfolk County Asylum (1814), Staffordshire County Asylum (1818), West Riding of Yorkshire County Asylum (Wakefield) (1818), [described as H form at the time],
RADIAL PLAN
Long wings radiating from a central (often semi circular) hub. Considered
inhumane even in its own time and only really implemented in the south-west
(other than prisons). The close nature of the wings at the point nearest
the hub would allow little access for air and light to the buildings and
airing courts between them. One source suggests this plan offered a
deterrent to potential admissions as asylum care would have been preferable
(and more expensive) to the workhouse. Eg. The main block at St. Lawrences
(Cornwall, 1820), and Exe Vale/Exminster
(Devon, 1845).
A radial plan with only two wings - radiating on the same diameter line,
either side of the hub - is a
corridor plan
CORRIDOR PLAN
Originally Corridor - A long running and variable group
1830-1890. They are
typified
by a (often projecting or recessed) central block including admin and
former officers quarters, flanked by long wings either side, each with
appropriate working areas and segregated by sex. Built to two or three
storeys in height. Typically (as the name suggests) a corridor or 'passage
of communication would run the length of the building to ease access.
Widespread across England and Wales.
Eglinton, Ireland
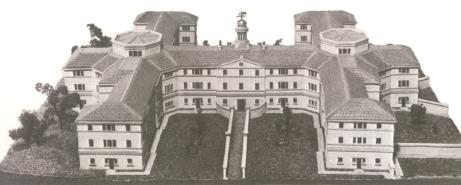
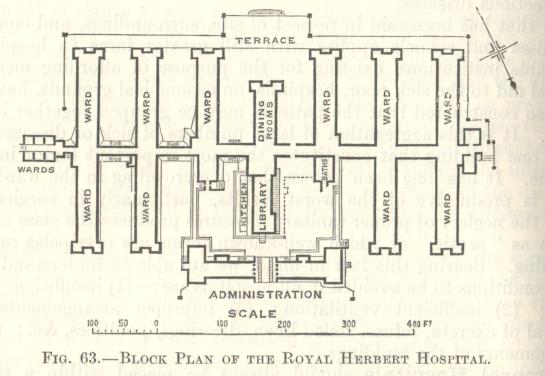
PAVILION PLAN
The first Pavilion type hospital was the Royal Herbert, on Shooters Hill
Eltham, a military hospital.
[Opened 1.11.1865. See
external link].
The second was St. Thomas' in London [opened 1871]. These were designed on principles recommended by Florence Nightingale. The Architect of Royal Herbert being her nephew. Therefore all pavilion and corridor-pavilion types should post-date these
Corridor-Pavilion: About 1870 to 1890. An ill-defined group of
buildings intermediate in character between the two types. Thanks to its
vague definition, I cannot really seem to identify many to this layout.
Possibly used at St. John's and St. Lukes (on a radial corridor) divisions
at Whittingham (Lancs), De La Pole (Hull). The first and last show a
courtyard type plan with wards facing into this area.
Pavilion - 1870 - 1907 (in asylums). A hugely widespread type, and
essentially the first common hospital plan and greatly advocated by
Florence Nightingale, but little used within asylum design.
The principles
of it seem to have been utilised in the echelon plan.
i, Standard Pavilion - Usually consisting of a long linear corridor with
individual ward blocks to allow free passage of air and light. Central
admin block. Hall and services could be central or remote. Eg. Hellesdon
(Norwich), Darenth Park (MAB)(original block and first annexe)
ii, Dual - Axial services and facilities flanked on either side by long
corridors with individual blocks. The sheer size of these complexes blocks
made them operationally difficult and they were initially intended as
somewhere to segregate incurables and chronic cases away from other
patients. Typified by the huge Caterham and Leavesden Imbecile Asylums of
1870 for the Metropolitain Asylums Board of London (which used the pavilion
plan in nearly all of its hospital buildings). Banstead 1877 (for
Middlesex) and Possibly Winwick (1897) may have been the only non-imbecile
examples. Calderstones Certified Institution 1905 (Lancs Asylum Board) is a
late example.
iii, Radial Pavilion - An oddity, and intermediate between the standard
pavilion and the development towards the echeon plan. Individual ward
blocks arranged around a semi circular corridor with axial office and
service accomodation.
Cane Hill (Surrey 1883) is the only true example but
could include
Whittingham's St. Luke's Block (which had remote services) in
some respects.
iv, Irregular - eg. The Manor Certified Institution (at Epsom for London
CC) was a large structure consisting of temporary pavilions arranged around
an L- shaped corridor, with a pre-existing mansion as its hub and offices.
Darenth Park 2nd Annexe consisted of two groups of five y-shaped pavilions
linked by corridors.
ECHELON PLAN
Echelon - 1880 - 1932. Largely superseded the
Pavilion plan of Asylums
in all but the Metropolitan and Lancashire Asylums Boards. Its sudden rise
in popularity being the arrangement of wards, offices and services within
easy reach of each other by a network of interconnecting corridors.
Typically forming a triangular, trapezium or semi-circular format.
i, Broad Arrow 1880-1890. The earlier form of echelon plan
consisting of the
typical layout with services and wards (segregated by sex) located on a
wide spreading complex. Broad Arrow wards were essentially detached
pavilion blocks linked by stubby corridors to the main corridor network.
Coney Hill (Gloucester 2nd) by Giles and Gough would have been the first
had it been completed to plan.
High Royds (Menston, West Riding) 1888 by J.
Vickers-Edwards was probably the best example.
ii, Compact Arrow
1890
- 1932.
This plan revolutionised the construction of
Asylums and Mental Hospitals and was probably the most practical type
devised. The linking corridors of the Broad Arrow were retained, but
instead the ward blocks 'hugged' the main corridors rather than being
placed away from them. Ward blocks could be either interconnecting or
distinct from each other. Typically these wards would give the appearance
of a zig zag as they were stepped along the main corridor. As in previous
designs, male and female workplaces would be located on their respective
sides with shared services and offices occupying the centre.
Later examples
had detached villas in the grounds for working, epileptic or chronic
patients, and also Acute blocks to avoid incorporation of recent cases to
the main building. Later developments towards
the Colony layout
included
some asylums with open sided corridors and ward blocks becoming further
detached.
Claybury
(opened 1893 in Essex for London County) was the first compact arrow
plan and was greatly praised in its time, becoming the model for asylum
design and its architect
GT Hine
becoming the most accomplished and
successful of asylum architects.
Bexley
(in Kent for London County),
Hellingly
(West Sussex),
Barnsley Hall
(Worcestershire) and most other Hine Asylums are based upon
Claybury. Other architects such as Giles, Gough and Trollope
(
Cheddleton County Asylum, Staffordshire)
and
Tone Vale
(Somerset), Vickers-Edwards
(Storthes Hall - West
Riding)
and many others adopted this principal for their works.
Park Prewett
(by Hine) is of the
later type with open corridors and separate
wards blocks.
Cefn Coed 1932 (Swansea Borough) seems to have been the last
example to be completed.
|
Landscapes:
Sarah's Rutherford's study (9.2003), The Landscapes of Public
Lunatic Asylums in England, includes
nine case studies of asylum history, architecture and landscape:
-
Moorfields Bethlem (1676)
-
The Retreat
-
Brislington House
-
Nottingham
-
Norwich
-
Wakefield
-
Hanwell
-
Derby
-
Middlesbrough
-
Ewell Epileptic Colony
The main thesis analyses the English public
asylum landscape during its development from
1808 to
1845, and subsequent consolidation and variation into
other related types during the main period of public asylum building (from
1845 to 1914).
It analyses the asylum as a distinct landscape type, its principal
influences and context, also the main design influences, particularly the
landscape of the country house estate. It also examines issues connected
with the conservation of this type of landscape, in the face of current
grave threats to the fabric. The work looks at the use of the asylum
landscape, concluding that its principal function was therapeutic. For this
it needed an extensive, ornamented landscape so that patients could
undertake recreational and work activities. A number of individuals were
found to have contributed to the design of various asylums, including
professional landscape designers commissioned to design asylum sites. These
included a previously unknown designer, Robert Lloyd of the
Brookwood asylum, Surrey, who was particularly prolific in this
field, and was associated with at least seven asylum sites.
in the early 17th century, the space in front (and behind?) the main
building contained a single airing court. A second court was added in an
expansion of 1643-1644.
By
the later 17th century Ogilby and Morgan's
map of London shows that there was virtually nothing of the formerly
spacious precinct left that had not
been built upon, apart from the limited space in front of and behind the
main buildings.
But by then it was set in a noisy, crowded location which did
not suit the aspirations of the City
of London or medical requirements for fresh air to combat infectious
miasmata.
Moorfields Bethlem - The landscape - 1676-1815
Until
the mid-eighteenth century, the
Moorfields Bedlam, designed by
Robert Hooke, was the
only significant example of a
purpose-built lunatic hospital in Britain. Major features of Hooke's
Bethlem, in terms of the setting,
accommodation and treatment, provided the model used for other charitable
lunatic hospitals founded in
the eighteenth century and even the publicly funded county asylums in the
nineteenth century. As such its
estate was very influential in asylum construction, including the principal
elements of the estate: the
building, airing courts and forecourt.
The new site selected,
close by Bishopsgate, at the head of Moorfields, was
chosen for its "health and aire",
the benefit of an ample, unsullied fresh air supply and its effective
circulation being regarded by the
Governors as the key to healthy surroundings.
The poem Bethlehem's Beauty (1676) emphasised the
perceived virtues of the new site's healing air:
Th' Approaching Air, in every gentle Breeze,
The Governors employed the prominent architect Robert Hooke (1635-1703),
who was actively involved in
the rebuilding of London after the Great Fire, to design the building.
Largely constructed by 1676, it was
probably only the third purpose-built asylum, after one in
Valencia (1409, destroyed 1512) and the
Dolhuys in Amsterdam (1562).
Andrews states, in connection with the intentions of the Governors, that
they were
The Moorfields Bethlem was in Lower Moorfields, to the west of Bishopsgate.
. Like Bishpsgate, it was outside the north boundary of
the City, although only just so. The site for the building ran parallel
to the ancient London Wall, and only
nine feet (3m) to the north of it, occupying open ground on the site of the
old City ditch which had been
filled in. The site formed the south boundary of, and overlooked,
Moorfields, a series of substantial formal
public open spaces laid out from 1605, which, although largely surrounded
by development, formed a
finger of open space which led directly out to the open fields to the
north.
Moorfields Bethlem was palatial in
scale, even in terms of new constructions put up as part of the building
campaign after the Great Fire,
being intended to accommodate 120 patients. The about 540 feet (166m) long
entrance facade on the north
front was depicted by Robert White in an engraving of 1677
(external link to picture), shortly after
construction, together with parts
of the grounds.
The single-pile building was of two storeys over a
basement, and showed Dutch and French influences in its elaborate external
decoration. The patients were
segregated indoors, at first with males on the ground floor and females on
the first floor. The cells, for
individual patients, led off galleries which served for communication and
for exercise in inclement weather.
John Evelyn was one of the many admirers of new Bethlem, describing it as
"magnificently built, & most
sweetely placed in Morefields". There must surely have been a service
entrance on the south side of the
building, between it and the City Wall, although the space between the two
was only nine feet (3m).
White's engraving clearly shows the grounds and part of the
provision made
for patient exercise.
The outline in plan form of the building and its open spaces in
relation to their setting is also shown
on contemporary maps of London such as Morgan's map of 1682
(external link to map)
The grounds were divided into a
large rectangular forecourt in
front of the building, flanked by two smaller exercise yards. The whole was
approached via the formally
laid out and enclosed lawns of Moorfields, a fashionable recreational space
for the local inhabitants which
had been one of the first such formally designated public open spaces.
Security at Bethlem was of great
concern, as patients were perceived to be continually likely to abscond as
the opportunity arose. As reliable
staff to supervise patients were difficult to find, the Governors had to
rely on making the environment itself
provide the means for ensuring confinement. The first three reports on the
construction of the building by
the hospital's Committee of Governors were largely taken up with matters
concerning the boundary wall
that was to surround the hospital and its grounds, and to confine the
patients.
The existing London Wall was used to form part of the secure 680 feet
(c.207m) long south boundary
wall. On the other sides a wall was to be constructed at 14 feet (4.2m)
high along the sections which
bounded the airing courts, with a coping expressly intended to stop the
lunatics escaping. The exception
was the front, north, wall of the forecourt which ran parallel to the whole
length of the building and divided
it from the adjacent Moorfields. This c.420 feet (c.128m) long central
section of the whole north wall
would be only eight feet (2.5m) high, so
The lowering of the forecourt wall did
not affect security, for the
patients were forbidden to exercise in the forecourt.
(Bethlem Royal Hospital Archives, Bridewell and Bethlem Court of Governors
Minutes, 23.10.1674)
The wall was broken
by six evenly spaced panels of
iron railings, each forming a ten-foot (c.3m) wide clairvoie intended to
enhance the views of the building
from the adjacent and impressively laid out Moorfields open recreational
space. The views were clearly
intended to impress the users of Moorfields, both nearby residents and
visitors alike, and the visitors to
Bethlem itself upon their approach.
The north side of the building and the forecourt are shown in detail on
White's engraving
, with a passer-by
admiring the ensemble. The clairvoie panels were flanked by piers
surmounted by stone pineapples.
At the
centre of the forecourt wall an elaborate triple gateway gave access from
the formally fenced and tree-lined
lawns of Moorfields to the north, between which the visitor approached. The
portentous gateway was
elevated above a flight of steps and surmounted by the
life-sized statues
of two figures depicting raving and melancholy madness,
attributed to Caius Cibber.
From here the visitor crossed the expensively paved
and gravelled forecourt to gain access to the main entrance at the centre
of the building. There were
numerous large windows in the north walls of the ward wings, flanking the
central administrative block,
allowing for the ample ingress of light and air. Those in the raised ground
floor and first floor, in
particular, gave the patients an elevated view of the forecourt, and beyond
this of the designed open spaces
of Moorfields.
The sites of the Bishopsgate Bethlem and the Moorfields Bethlem are shown
on the sketch map
Robert Hooke's architecture (Moorfield's
Bedlam)
Robert Hooke was a close colleague of Christopher Wren and
designed several
other
institutional buildings in London
including the Bridewell Hospital (1671-78), also for the City of London;
the Haberdashers Aske's Hospital, an
almshouse at Hoxton (c.1690-93); with John Oliver, Christ's Hospital
Writing School (1675-6); as well as several
town and country houses. Hooke's Hoxton building was of similar design to
Bethlem: a long, single-pile building
with an elaborate central block connected by flanking wings to two
pavilions. A large, grassed forecourt appears to
have been used by the inmates for recreation and exercise, and was divided
from the road beyond by a wall and
central gateway, the whole layout in similar formal style to that at
Bethlem. It is illustrated in Strype's edition of
John Stowe's Survey of the Cities of London and Westminster (1720). Hooke
only used the single-pile design for
these two hospitals, not for his houses.
Is Fan'd and Winnow'd through the neighbouring Trees,
And comes so Pure, the Spirits to Refine,
As if th' wise Governours had a Designe
That should alone, without Physick Restore
Those whom Gross Vapours discompos'd before
"much more concerned with the 'Grace and Ornament of the _
Building' than with the patients'
exercise or any other therapeutic purpose - New Bethlem was constructed
pre-eminently as fund-raising
rhetoric, to attract the patronage and admiration of the elite, rather than
for its present and future inmates,
whose interests took a poor second place'"
"that the Grace and Ornament of
the said intended Building may
better appeare towards Morefeilds"
| Bethlem exercise courts | after the 1730s |
The boundary wall also enclosed the two exercise yards, which flanked the forecourt at the corners of the building. The forecourt was several times larger than either of the exercise yards, which were limited in their extent by, apart from the forecourt which divided them, the proximity of Moorfields to the north, the London Wall to the south, and development to the west and east. Two yards were provided "reserved for the use and benefitt" of the inmates, one each for the separate sexes to exercise in. Those patients "well enough" were "permitted to walke the Yards there in the day tyme", so that they could "take the aire in order to [aid] their recovery". (Bethlem Royal Hospital Archives, Bridewell and Bethlem Court of Governors Minutes, 23.101674 and 5.5.1676, and Bethlem Committee report, 16.10.1674.
Each yard was surrounded by the 14 feet (4.2m) high wall, topped with a "Coping _ intended to p'vent the Escape of Lunatickes". Both were laid out with grass and gravel plots of 120 feet (36.5m), with, set into the rear wall, a small pavilion with windows at first-floor level. (Bethlem Royal Hospital Archives, Bridewell and Bethlem Court of Governors Minutes, 23.10.1674 and White's engraving 1677
The upper level of the pavilions may have provided shelter for attendants supervising patients whilst allowing them an elevated view of their charges in the yard, with the lower level providing shelter for the patients.
| Bethlem airing courts after the 1730s | before the 1730s |
By 1786, Bethlem was noted for its "fine gardens" where the patients "enjoy fresh air and recreate themselves amongst trees, flowers and plants".
Although there was no formal classification by symptoms, there was obviously a category of patients who were allowed to exercise outdoors. Those whose behaviour was deemed to be too wayward or who were physically too unwell remained indoors.
By 1740 the wings had been extended to west and east in L-shaped form, covering much of the site of the early airing courts. Provision for patient exercise was made by reducing the width of the forecourt, such that it only extended half way along each of the original wings. It had also lost the clairvoies formerly sited in the north boundary wall. The open ground formerly flanking the forecourt was given over to airing courts, surrounded by higher walls. The old gateway had been re-sited to the south, much closer to the front door and a curved carriage sweep open to Moorfields now provided more direct access to theentrance to the building, while dividing the forecourt into two compartments. This removed the need for visitors to cross the forecourt on foot to gain admittance. The opening up of the approach physically linked the main entrance to the building with the main axial walk of Lower Moorfields pleasure grounds.
The Moorfields site was abandoned in 1815, when a new site was opened in St
George's Fields,
Southwark. The old building had for long been unsound, having been
constructed very quickly of poor
materials over the unstable infilled ground of the City ditch below the
City wall. The building was
demolished and Finsbury Circus was developed on its site.
Elements drawn from
Bethlem were used at the core of both The Retreat and
Brislington House: These being principally
the airing courts.
The use of moral treatment was manifested in the construction
of further, new elements in the wider landscape.
Samuel Tuke described the grounds and the building, which had been designed
by a London architect and
builder, the Quaker John Bevans. Bevans had designed a number of other
buildings for the Society of
Friends including several meeting houses. The brick building, which by 1813
held 50 or so patients, was
said by Tuke to be designed chiefly for economy and convenience. However,
the layout of the building was also intended to facilitate the
classification of patients in various ways: by gender, social class and by
clinical state. The so-called quiet
patients, those exhibiting non-disruptive symptoms and those being
convalescent, were separated from the
disturbing and disruptive behaviour of more refractory patients. The
division by gender and by clinical
state was manifested in the layout of the building and in the associated
airing courts. Two ward wings, for
the more tractable category of male and female patients, extended in
opposite directions from the central
block and benefited from airing courts adjacent on the south side, and the
associated views out over the
walls to the surrounding countryside. The two courts were divided by a
central path giving access to baths
at the back of them. A semicircular wall, which marked the outer boundary
of the two inner courts for the
more tractable patients, was about eight feet (2.4m) high "but, as the
ground declines from the house, their
apparent height is not so great; and the view from them of the country is
consequently not so much
obstructed, as it would be if the ground was level"
The two main wings led in turn to two smaller wings, almost entirely
detached from the main building,
with associated walled airing courts. Here were housed the more refractory
class, who could be noisy,
unclean in their personal habits, and violent. Because of such antisocial
behaviour, physical isolation was
practised in order to reduce their negative effect on the other patients
and localise the amount of extra work
which they created for the staff. Each of the four airing courts covered
between four and five hundred
square yards (334 to 418m sq.).
For those patients too physically ill or difficult to control to be allowed
beyond the confines of the courts,
the courts were supplied with domestic animals as pets including rabbits,
sea-gulls, hawks and poultry.
Samuel Tuke censured the courts as being too small and confined, this, he
believed, being deleterious to the
patient's state of mind when the boundary of confinement was always so
obvious. However, the sense of
confinement, he said, was alleviated by taking such patients as were deemed
suitable into the garden, and
by frequent excursions into the city or the surrounding country, and into
the fields of the Institution, one of
these being surrounded by a walk, interspersed with trees and shrubs [in
the manner of a ferme orn�e]. The
criteria for being regarded as "suitable" for these activities related to
physical robustness and whether or not
the patient's behaviour was considered to be too antisocial or whether they
could conduct themselves with a
reasonable measure of self-control.
The French doctor Charles-Gaspard de la Rive published a useful early
account of The Retreat in the
Biblioth�que Britannique following his visit in 1798. It suggests that he
had an agreeable surprise at the
pleasant conditions of the asylum, although Foucault believed that the main
purpose of the institution was
to serve as a repressive instrument of segregation. According to de la Rive
it lay, "in the midst of a fertile
and smiling countryside; it is not at all the idea of a prison that it
suggests, but rather that of a large farm;
it is surrounded by a great, walled garden. No bars, no grilles on the
windows".109 It had 11 acres (4.5 ha.)
of land and was largely given over to growing potatoes, and grazing cows
which provided milk and butter
for the establishment. A one-acre (0.4 ha.) kitchen garden lay to the north
of the building and provided
abundant fruit and vegetables which fed the establishment.
The Retreat also provided a place for recreation and employment for many of
the patients, "being divided
by gravel-walks, interspersed with shrubs and flowers, and sheltered from
the intrusive eye of the
passenger, by a narrow plantation and shrubbery".110 The clothing of the
grounds was apparently a major
feature; fourteen pounds and ten shillings-worth of native and exotic woody
plants were bought in 1794
from the notable York nurseries of John and George Telford, and Thomas
Rigg, at a time when the
erection of the building was hardly advanced.111 For this amount 768 plants
were purchased.
The asylum building was therefore surrounded by the equivalent of a small
country estate, with ornamental
pleasure grounds, and productive kitchen garden and farmland. It fused the
elements which were purely
asylum-related with the type of carefully constructed country house-type
landscape that was being
promoted by landscape improvers and designers such as Humphry Repton (1752-
1818)
Brislington House was the first purpose-built private asylum (1804-1806)
Its proprietor,
Dr Edward Long Fox (1762-1835), was a Quaker, and the
structure and regime were almost certainly influenced by
The Retreat. Brislington House
reflected the layout of the site at The
Retreat, while extending, developing and increasing the individual
elements. Its patients were mostly wealthy, members of the gentry and
nobility, but it took some paupers.
The influence of Fox and
Brislington House extended widely in England and Scotland and was
influential on the erection of the county asylums..
The
text of his (about) 1806
promotional pamphlet for Brislington House was reproduced in full with
Robert Reid's Observations on
the Structure of Hospitals for the Treatment of Lunatics (1809), which was
published together with Reid's
proposed designs for the new
Edinburgh asylum.
Fox's pamphlet was quoted as
being a "valuable authority" in the second edition of William Stark's
Remarks on the Construction of Public Hospitals for
the Cure of Mental Derangement (1810). Here Stark republished his proposals
for the construction of
Glasgow asylum, and expressed his regret at not having known of
Fox's
pamphlet for the first edition in
1807, as "it would have supplied me with much valuable authority respecting
many of the statements
contained in my former Report".
Fox's asylum arrangements continued to be
directly influential for some
years.
On
29.4.1828 Edward Fox petitioned the House of Lords against the
provisions of the Madhouses Bill. Fox gave
extensive evidence to the
1828
House of Lords Select Committee
Inquiry relating to lunatics and asylums. His asylum may
additionally have
been influential because of
the number of influential and wealthy people who visited their relations
when patients there. Even in the
1830s W.A.F. Browne commended favourably in print upon the structure of Dr
Fox's Brislington House
and his therapeutic regime.
By the late 1820s Dr Fox accommodated "all Classes of Society" at
Brislington House, but there were very
few pauper lunatics. Classification was as important as in the early days
of the institution, "Not only are
the Classes of Society kept distinct, but three Classes of each Society are
kept distinct according to the
State of the Disease". There was also division by sex. To effect this
classification, the establishment was
divided into six "houses", with two attendants for each one. One other
house was provided, for paupers,
detached from the main group. In terms of cures effected, in 1826 Fox
received 42 patients, 22 of whom
were cured and nine were under gradual improvement; one was discharged to
another asylum, five died,
and the remainder continued at Brislington. There were on average 90
patients in the asylum.
The building stood at the heart of the site, with an open and informal
forecourt to the front and a block of
rectangular airing courts to the rear, and views from the rear towards the
distant Bath Hills. Its six
separate ward pavilions, referred to by Fox as "houses", comprised three
for males and three for females
flanking a central block.
Initially the patients were classified by social rank, then by severity of
symptoms, rather than by type of
illness. Those of the highest social rank were referred to as "ladies" and
"gentlemen", and were allocated themost prestigious accommodation within
the upper floors of the main central block (divided into two for the
separate sexes). The lower ranks comprised males and females of the second
and third classes who
inhabited the two larger pavilions of the three on either side of the main
block. The various social classes
and sexes were never to meet. The accommodation was graded such that the
central block, where Dr Fox
himself lived, was for the higher class, the central two of the flanking
pavilions were for the second-class
patients, whilst those furthest from the main block were for the third,
lowest class. The smallest of the
three pavilions on either side of the main block was for use as an
infirmary or isolation block.
An unusual management and treatment feature was the manner in which a line
of cells was sited at the far
end of each of the airing courts at the back of the building. These
isolation cells, for the more recalcitrant
patients, were placed well away from the ward pavilions so that those
patients who were quieter and less
disruptive were less disturbed by noisy patients. However, they were still
within call of staff and services
from the main buildings. The main building, cells and courts were enclosed
by a wall and the only entrance
and exit, apart from the doorway to the walled garden behind, was via the
main central door opening onto
the forecourt.
On the front, entrance side of the building lay an informal forecourt with
a grand turning circle. This was
divided from the main house and its individual ward blocks by two outdoor
sunken service passages to
allow communication between the blocks, which also flanked and linked with
the central block. To prevent
escapes these passages were divided from the forecourt and wider estate by
a stone wall 11 feet (3.5m)
high.
Behind the ward pavilions lay the line of six walled airing courts, to
which Fox said, patients had access
"whenever they please". Each of the three social class divisions within
each sex was specifically allocated
one of the courts. Those two for the second class were a few feet broader
than those for the other classes,
and the "gentlemen's" court had direct access to the walled garden behind.
Each court contained lawns,
paths and a central viewing mount to allow the patients views over the
countryside to distant hills. The
provision of these mounts was a novel feature designed by Fox. A border
sloping towards the outer wall of
each court in the form of a ha-ha prevented them from escaping, while
allowing a good view of the
surrounding country.28 In general the courts resembled domestic town
gardens, where the emphasis in each
enclosed space was on combining rural views, if available, with ornamental
and convenient amenities for
recreation. The therapeutic use of airing courts had not been classified to
such a degree before. Neither, it
seems, had their layout been so elaborate or provided with features
allowing the patients to take advantage
of "therapeutic" views. Brislington House, along with The Retreat, was one
of the earliest asylums to
promote the enjoyment of the surrounding setting of the asylum for
therapeutic purposes. It is clear that Dr
Fox, as part of as his aim of curing via moral therapy, constructed these
core elements, building, airing
courts and walled garden, to ensure that those patients whom he considered
required confinement were not
allowed the opportunity to escape.
Beyond the airing courts a bowling green and fives-court were provided, and
other "innocent amusements
for exercise" were allowed, probably largely for the higher social classes
of patients.30 In order to provide
ample recreation and employment facilities, and because Fox did not want
patients to be disturbed, or
incommoded by neighbours complaining of disturbance, the asylum was sited
in 80 acres (32 ha.) outside
Bristol on an isolated tract of former common heathland. The main buildings
stood at the centre of what
amounted to an extensive and purpose-built country house estate with
modifications for use in the
treatment of lunatics (Plate 27, annotated plan of estate, 1902). The
traditional country estate elements,
parkland, pleasure ground, lodges, approach drives, and kitchen garden, all
enclosed by a stone wall, were
supplemented with secure, walled airing courts adjacent to the main
buildings. Additionally, a number of
cottages were erected in picturesque style around the grounds, in a manner
reminiscent of Blaise Hamlet
(c.1810), built nearby on the west side of Bristol to designs by John Nash.
The patients' cottages, scattered
in the park in their own small grounds, were for the most wealthy patients
who could not be accommodated
in the main block in the style to which they were accustomed (for example,
see Plate 24, the Swiss
Cottage, built in 1819). In this way they could live, with their own
retinue if desired, splendidly isolated
from all possible social and medical taint associated with the main asylum
buildings, while benefiting from
the proximity of the expert Dr Fox and his establishment.31
Several passages written by John Perceval concerning his enforced stay as a
patient at Brislington House
in 1831 address the uses to which this early therapeutic landscape was put.
Although Fox was initially
reluctant to give gentlemen activities below their perceived status,
Perceval's narrative indicates that
gentlemen were allowed to work in the gardens and grounds of the House.
Perceval complained that upon
his admission in January 1831 there was little for him to do indoors, apart
from looking out of the window
and reading the newspaper. His mother asked Dr F.C. Fox to let Perceval
work in Fox's garden "this was
indeed beneficial, as it gave me occupation and more privacy". Later on in
the year he was employed with
two other gentlemen and an attendant to do further work, cutting out a
small path in the shrubbery, having
been entrusted with a mattock and spade, although he rejected these when
his voices teased him with
contrary instructions, reverting instead to wheeling the barrow, picking up
sticks and using a bill-hook.
Perceval refers to the use of the airing courts, or yards, for exercise and
a change of scenery, as a common
activity for patients, used together with walks further afield within and
outside the grounds. Seats were
provided, and patients might be left on their own, "When left alone in the
yard, [a patient] amused himself
with picking up stones, climbing up into a small tree and sitting there
looking over the country, and one
day he picked nearly all the leaves off this tree".33 Later on in the
1870s, the Reverend Francis Kilvert
recounted in his diary visiting his aunt Emma who was to be found sitting
in the gardens, doing some work
with a cat or two on her lap, where they walked whilst talking.34
Perceval describes a precipitous pleasure ground known as The Battery,
situated on a terrace above the
River Avon, to which the patients were often taken, and its drawbacks for
those experiencing hallucinatory
voices. "At one elevated spot that commanded a view down the valley, a
natural or artificial precipice
yawned in the red soil, crowned with a small parapet, in rear of which was
a small terrace and summer
house [the Battery]". The view was, apparently, enchanting. A photograph
shows the picturesque
summerhouse at the turn of the century.35 Here Perceval sat on the parapet,
overlooking the precipice, "My
voices commanded me to throw myself over, that I should be immediately in
heavenly places" and having
managed to resist this injunction, on subsequent visits he refused to go up
to the parapet, but instead sat in
the summerhouse "to avoid the temptation". Other patients sat on the
Battery, but Perceval disapproved of
them being taken there at all for safety reasons.
The asylum continued to be owned and run by the family until c.1950, when
the asylum building was sold
to the NHS as a nurses' home. Following a period as a nursing home in the
1990s it has been converted
into private apartments, and a school built in part of the park.
The first publicly funded county asylum to open under the 1808 Lunatics
Act. Laid out before
patients were widely considered
to benefit from a regime of exercise, recreation and employment. The two
subsequent asylums constructed under the 1808 Act
(Bedford, 1810-1812 and
Norwich 1811-1814) had buildings and estates largely arranged in
a similar fashion.
In 1808 just under five acres (2 ha.) of land were purchased at Sneinton on
the south-east edge of
Nottingham. The asylum was set at the edge of a rapidly expanding urban
area
and took patients from both
rural and industrial areas. It was constructed initially as a relatively
large establishment for 60 patients.
In 1809,
Nottingham Magistrates sought advice from Dr Fox of
Brislington House about the the asylum and the layout of the asylum
grounds. They were
principally interested in his novel building layout of divisions into
separate blocks (which they did not
ultimately act upon), presumably because they were interested in systems of
classification. Fox also
advised on other matters including the grounds immediately surrounding the
asylum building.
(One of the
magistrates who contacted Fox was the Rev John Becher of
Southwell). (Nottinghamshire RO,
SO/HO/1/1, Nottingham asylum, Committee minutes, entries for March and
April 1809)
It was stated in the 1814 Annual Report that from the outset a "liberal
spirit" suffused the intentions of the
asylum governors, such that by their Fourth Annual Report of 1818 they
could state that, "they have seen
that the system adopted in your Asylum is invariably that of tenderness and
gentleness, united with a firm
and powerful resistance against maniacal paroxysms, yet restraining and
coercing the unhappy patient no
longer than the occasion may require". The liberal spirit was obviously
tempered with a perceived need
for practical restraint at times.
The 1818 Annual Report also related the purchase in the previous year, and
at the considerable expense of
£700, of a parcel of land behind (that is, to the east of) the
asylum. There were three reasons given for this
acquisition, which was considered to be of considerable importance to the
welfare of the asylum. The steep
slope of the land down from the east allowed passers-by to overlook the
asylum and its airing courts,
causing "very great annoyance, which was too frequently found to harass and
disturb the minds of the
Patients placed in those Courts for air and exercise, and to retard their
recovery". The new parcel of land
created a visual barrier to the inquisitive who had no business looking
into the asylum grounds. The second
reason given for the acquisition of this land was that, "it is obvious,
that more extensive means of
employment will thus be furnished for such of the male patients, to whom
bodily labour may be deemed
serviceable". This is a very early example of the managers of an asylum
declaring the therapeutic benefits
of employment. It appears that the employment of patients had already been
contemplated and possibly
carried out, and the original extent of land not found to be great enough
to allow all those to work who
wished to or were able. The final reason for acquiring the land was that
"in the cultivation of this ground,
considerable benefit will be derived to the Asylum". This probably referred
to its economic use to provide
fruit and vegetables for the institution.
Richard Ingleman designed
a building which followed the general plan form of the
Moorfields Bethlem, with men and
women's wings flanking the
central administration and service block. The asylum
was built as one long, three-storey block, with galleries overlooking the
airing courts to the rear. The
asylum was set 300 feet (92 m) back from the road. The building and airing
courts were set within a
tightly drawn walled enclosure (248 feet x 348 feet; 76 x 107m), behind an
area of informal lawn which
was obscured from the road by a screen of trees (see Plate 30, annotated
plan of the estate, based on the
OS 25" plan, pub. 1883).95 A lodge, costing £390, was erected at the
same time as the tree screen was
planted in 1809, even before the committee could afford to put up the
hospital building.96
From the lodge a serpentine drive was cut through the hillside, crossing
the lawn to the turning circle in
front of the asylum building. Dr Fox in 1809 advised that the approach to
the asylum should prevent
patients from seeing the asylum, from seeing visitors to the asylum, and
from being able to guess its
purpose. The asylum did not have a farm attached, but the lawn at the
front, encircled by woody planting
in the manner of an informal pleasure ground, may have been used for
supervised patient recreation.
Fox advised that instead of the three airing courts per side, which his
establishment had, probably only two
airing courts each for the male and female sides were required, one
designated for the "filthy and
refractory", and the other for the "temperate cleanly and convalescent
patients". The building and courts he
recommended should face somewhere between the east and south-west, the
whole being arranged so as to
prevent communication between the sexes by speech or otherwise. Three
airing courts per side were
subsequently built, with a gap between the two central ones to provide
access from the central
administration block to the kitchen gardens beyond.99 The airing courts on
male and female sides each
seem to have been assigned to a different medical class of patient.
In 1828 Halliday referred to the asylum. He expressed his dissatisfaction
with the amount and use of space
for patients to be employed within. He believed that there was 4.5 acres
(c.1.8 ha.) of land attached to the
building, which could take 80 patients. "The land is laid out as a garden,
the cultivation of which is the only
employment the patients have. Their treatment however, seems to be well
conducted, and the strictest
economy preserved, as the expense of each person does not exceed
7s./week".
Some time after 1844 the building was extended, and the airing courts, of
which there were now seven,
were remodelled and thrown into two large main courts, with a third
alongside to the south. The courts
were terraced to accommodate the steep slope up to the east and laid out
with lawns and paths. The land
beyond the courts was laid out as an elaborate terraced garden with wooded
zig-zag paths connecting the
main terraces at the top and bottom. Seating areas were provided at the
back of the upper terrace,
overlooking the asylum grounds below, and a fountain at the centre of the
lower terrace. The setting
became more built up, with networks of streets with small houses to the
west and south, although open
ground remained to the north, and to the east lay large areas of detached
town garden plots and other open
ground.
In the early 1900s the asylum was superseded by the new asylum at
Saxondale, and was closed and
demolished. The grounds were reused as King Edward Park.
One of the
magistrates who contacted Fox was the Revd. John Becher of Southwell).
Becher was active in other
schemes of social provision and classification, for in 1808 a workhouse had
been erected in Southwell to
his design, for 84 pauper residents of the parish, which was, as he
maintained, "constructed and governed
upon a principle of Inspection, Classification, and Seclusion".92 Becher
piloted and also helped to design its
even larger and more influential successor at nearby Thurgarton in 1824
(discussed in more detail in Chapter 4 of Sarah's thesis).
Norwich asylum was built three miles or so (5km) east of the city at
Thorpe. The individual airing courts
were laid out with gravel paths and grass plats, and were enclosed by 13-
foot (4m) high brick walls which
had to be raised once the first patient had escaped over them in 1814. As
with Nottingham, the two central
courts were divided by a narrow passage, this time flanked by an arcade
leading to the hospital buildings
for men and women respectively, each with its own small airing court. The
asylum was approached via a
walled forecourt with railings flanking gates leading straight off the
Yarmouth turnpike road which lay
close by. The remainder of the grounds were given over to a cemetery,
kitchen garden and drying ground.
The cemetery was laid out in 1815 at the south-east corner of the airing
courts, enclosed by a four and a
half-foot (1.5 m) high wall and consecrated by the Bishop of Norwich on 4
August 1815.
A lengthy description of the asylum in 1825 presents a very positive
account of the establishment and its
management. The writer described the situation as being "on a fine, open
healthy spot, near the Yarmouth
Road", approached via four iron gates set into cast-iron palisades on low
brick walls which gave access to
the "fine, open yard" in front of the building. He writes approvingly about
the arrangements for the patients
within the building. The airing grounds were reached directly by the
patients via their day rooms and
galleries on the ground floor, each wing (one for each sex) having three
areas, which the writer classified
as an airing ground, a probation yard, and a convalescent yard. The
description does not mention how the
patients were classified within the accommodation in the building itself,
although the men occupied the
west wing and the women the east. Each yard was enclosed by walls high
enough to "insure the safety of
the patients during the hours of recreation", and laid out with grass
panels intersected by gravel walks
which gave them a "neat and pleasant appearance". The male and female yards
were separated by a
semicircular courtyard, as shown on Stone's 1816 plan, from which a passage
led south to the other
offices. The court contained an arcade which continued along the passage,
leading on the west side to the
men's hospital, the nurses' room, a drying room and a stoving room. A yard
was appropriated for the use of
the hospital patients. On the east side of the passage was a similar
arrangement for women, with the yard
being used by convalescents. The author also mentioned the remaining part
of the site being appropriated
for a "burying ground", spacious kitchen garden, coach house, stables and
other offices.
In the early years of the asylum little written reference has been located
to the patients using spaces
outdoors anywhere other than the airing courts. Halliday's brief
description of 1828, as part of his countrywide
survey of asylums, referred critically to the asylum in terms of the amount
of space for patients to be
employed within. "It has not the advantages to be derived from a farm or
great extent of garden, but upon
the whole, is a well-arranged and ably conducted establishment".
The original five-acre (2 ha.) site was not greatly extended until the
1840s, after the Metropolitan
Commissioners in Lunacy had complained in 1843 about the seats and benches
in the airing courts being
furnished with chains and leg locks, and the inadequate extent of land
which they viewed as so essential to
the occupation of the patients.83 By January 1846 the Commissioners
reported that a considerable number
of men were employed in the yards and outhouses and the grounds and
gardens. Two and a half acres (1
ha.) of land was bought in 1847, providing a total of seven and three
quarter acres (3 ha.) for the use of the
patients, the new land being laid out partly as a garden and partly as a
pleasure ground intended for the
women patients to enjoy air and exercise
The building was extended by the county surveyor, John Brown c.1849 and the
male and female sides were
reversed to east and west respectively. The original arrangement of six
airing courts was remodelled to
form two large airing courts, one on each side of the south front, with two
new courts to the west and east
of the building. At that time a large, square kitchen garden lay
immediately to the west of the main
building, with a further area of kitchen garden to the east, and to the
north of this an area labelled "garden"
containing what appears to be an orangery or similar structure. The
cemetery, the narrow Governors'
Garden, the Drying Ground and Bowling Green formed a narrow band of open
land which separated the
hospital from land running down to the river to the south.85 At the same
time or shortly after, the turnpike
road was moved further away to the north to allow more room for expansion
and create more privacy from
the public road. Because of this the main entrance and lodge were
demolished and new lodges were built.
Following the re-routing of the road in a cutting, in 1856 a new and
substantial bridge, also by Brown, was
erected across the road, allowing male patients unhindered access from
their accommodation on the east
side of the site to the farmland to the north of the road.86
By 1854 there were 298 patients, and a further 30 acres (12 ha.) of land
had recently been bought, in
response to further criticism by the Commissioners in Lunacy and their
recommendation that this
constituted the minimum amount required for an asylum containing up to 300
patients. It was hoped that
the general increase in the space available to patients would lead to a
lessening in the number of chronic
patients and the lessening of the mortality of the other patients. The
exact use of the land had yet to be
decided, whether the more general activities of farming would be carried
out in addition to "spade
husbandry". It was believed that, "The more varied and extensive the
occupation of the patients, the more
fully will be developed their individual capabilities".87
The 1854 report admitted that the limited amount of asylum estate land had
until then made it difficult to
find work for those patients used to agricultural work. Idleness was
regarded as a major limiting factor to
the recovery of the patients. In the summer a piece of land had been rented
and 50 men were engaged daily
in "cricketing" and after that a large number were employed on the land;
however, nearly all the patients had
some kind of physical ailment, restricting the amount of work they could be
expected to undertake.
Marching drill occurred in the grounds, as "Great control is gained over
the patients, and the task of taking
a vast number to a distance from the Asylum for air and exercise, becomes
comparatively easy".
A self-contained annexe for 280 "quiet" cases of each sex was built c.1878-
80 at some distance to the north
of the original complex, on 24 acres (10 ha.) of land bought for the
purpose. This New Asylum stood
remotely in a large expanse of agricultural land and was provided with
airing courts which were enclosed
by sunken fences. The old and new complexes were connected by a sunken
drive across farmland which
left the turnpike road opposite the lodges. The old path which had
connected the two sides of the site since
the 1850s, carried by the bridge across the turnpike road, had been planted
up as an avenue. At the south
end of the path, in 1891-1892, the superintendent's house was built, set in
its own spacious grounds to the
east of the path. In 1899 all the male patients were moved to the New
Asylum and all the female patients to
the Old Asylum. In 1900 13 acres (5.25 ha.) were bought, and the New Asylum
extended for a further 150
patients. The southern, earliest part of the asylum closed in the late
twentieth century, and the building was
converted into apartments.
The Wakefield asylum was the earliest public asylum to introduce the use of
work in the building and
grounds at a significant level as a form of therapy, reflecting the
increasing interest in moral therapy in
public asylums. As such it was influential on other public asylums. Its
first medical superintendent,
William (later Sir William) Ellis implemented this programme, the asylum
having been constructed on an
expansive site with advice from Samuel Tuke of The Retreat, York, where
work was already a major
element of treatment. Tuke expressed his opinions on the laying out of the
asylum structure in print, and
the plans for the asylum were also published.
The Retreat - The landscape
"These creatures are generally very familiar with the patients: and it is
believed they are not only the means
of innocent pleasure; but that the intercourse with them, sometimes tends
to awaken the social and
benevolent feelings."
Brislington House - The Landscape
Nottingham - The landscape
1808-1836: Southwell Parish Workhouse
1824 to present: Thurgarton Hundred Workhouse, which
became Southwell Union Workhouse in 1836 (Now a museum)
Southwell workhouse open to the public
See Peter Higginbotham's site
PAPHE website
Norwich - The landscape
Wakefield - The
landscape
Hanwell - The landscape
|
|
 Study
links outside this site
Study
links outside this site
 Picture introduction to this site
Andrew Roberts' web Study Guide
Top of
Page
Picture introduction to this site
Andrew Roberts' web Study Guide
Top of
Page
 Take a Break - Read a Poem
Take a Break - Read a Poem
 Click coloured words to go where you want
Click coloured words to go where you want
Andrew Roberts likes to hear from users:
To contact him, please
use the Communication
Form
asylums index
Bethlem:
Brislington House:
Conolly 1847:
Corridor: -
Corridor-
Pavilion -
criminal lunatics
Derby:
Echelon: -
Broad Arrow -
CompactArrow -
Later Type
Ewell:
Landscapes
France (Ivry, Charenton, Rouen,
Vanves)
Hanwell:
Jacobi 1841
asylum situations
-
arrangement of departments
-
licensed houses
Middlesbrough:
Landscapes
Norfolk:
early - developed into corridor plan -
Landscapes
Nottingham:
early - developed into corridor plan -
Landscapes
Pavilion:
Corridor -
Standard -
Dual -
Radial -
Irregular -
Echelon
Retreat:
Landscapes
Wakefield:
Bishopsgate:
Moorfields:
original airing courts
1730s airing courts
St Georges
Jacobi form -
functions -
early colony plan? -
Landscapes
one of models -
ideal
features -
table -
functions -
Landscapes
Jacobi form -
Corridor plan -
functions -
Landscapes
forms -
model used?
Jacobi form -
developed into corridor plan -
functions -
Landscapes